I’m halfway through my two-week test, and thought I’d provide a quick progress report.
It has been both easy and hard to eat this way. Easy, in that I’ve certainly never been hungry. Hard, in that I’ve already gotten very bored with the things I can eat. (This is only because I’m a picky eater; there’s not much that I like. Especially, there are very few vegetables that I like. Eating a lot of eggs and meat, together with a lot of the exact same vegetables every day, has gotten quite tedious.)
I felt subpar on day two and the first half of day three: logy and tired. Several people suggested that the problem was probably not eating enough calories, so I tried boosting the size of my meals. Whether it was that, or just making it through the transition, I got over it easily enough.
I’ve done pretty well at sticking to the diet, with one exception: Easter brunch. I did fine for the salad course and the main course, but when they brought carrot cake for dessert, I was unable to resist. (Surely the carrots counteract the sugar, right?)
It tasted good, but very quickly I felt terrible. As I described in email to a friend, I assume what happened is this:
The sugar hit my blood stream, and all my carb-depleted muscle and liver cells said, “Oooh! Sugar! We gots to get ourselves some of this!”
But at the same time, my pancreas said, “Hmm. There’s sugar in the blood. I’ll release some insulin.”
But, because there was only one small serving of cake’s worth of sugar, in no time it was all gone. But the insulin was still there.
So my blood sugar plummeted.
And then my liver said, “But, but, I just got this teeny little bit of glucose! I haven’t even turned it into glycogen yet!” and then said, “Oh, all right. Here’s enough sugar to get your blood levels back to normal.”
I probably exacerbated the whole thing by going for a run—I thought of it as penance for failing in my commitment to be low-carb for two weeks. The run no doubt put additional pressure on my blood sugar levels.
Anyway, for a couple of hours there after lunch, I felt sick to my stomach, shaky, jittery, and had an inappropriately high heart rate. Some of that might have been psychosomatic, but it was all very unpleasant.
After my run I had a V8 juice, which may have helped. A tiny bit of sugar.
Except for that piece of carrot cake, my only deviations have been:
- Occasional small servings of cured meat (bacon, ham, sausage), which are generally low carb, but which are off the list for the two-week test because so many are cured with sugar or otherwise include carbs. I’m trying to pick ones that don’t have sugar, but am generally trusting that my servings are small enough that it doesn’t matter much.
- Some small servings of peanut butter, which is also off the list for reasons I don’t understand. It’s natural peanut butter with no added sugar, but of course peanuts do have some amount of carbs. Again, I’m keeping my servings small.
In my post saying I was trying the low-carb thing I had a list of specific issues I was hoping low-carb eating might improve: allergy symptoms, high blood pressure, high blood sugar, and weight. Taking those in reverse order . . . .
Weight
I can certainly see why low-carb diets are popular for weight loss: I lost several pounds almost immediately.
From what I’ve read, I gather this is largely water weight. Supposedly there are several grams of water bound up in the storage of each gram of glycogen. As the glycogen goes, the water is freed up, producing near-instant weight loss.
That all happened in the first two days. In the next five my weight has continued to trend down, but only very slightly. I assume this is mostly fat. If the second week is like the first, I’ll probably have lost about two-thirds of a pound of fat during the course of the test.
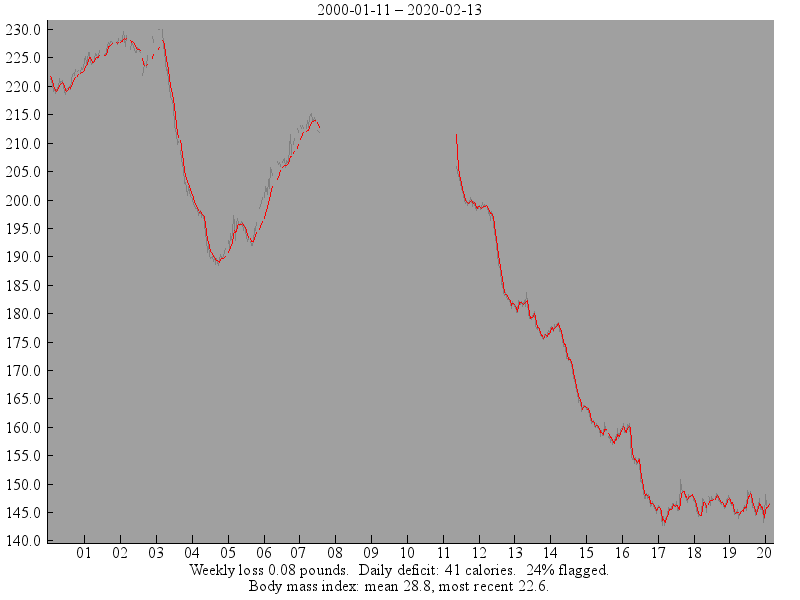
The dramatic weight loss is kind of interesting. Because I was already near my lowest adult weight, this big drop punched me down to a series of new all-time lows. I don’t have good data, but as best I can recall I am now at my lowest weight since I was a freshman in college and lost a bunch of weight when I had mononucleosis.
I assume those water pounds will pop right back on the instant I eat enough carbs to replenish my glycogen stores. That’ll be okay.
Blood sugar
I don’t have (and am not inclined to buy) equipment to check my blood sugar, so I don’t know if my fasting glucose levels are down or not. Empirically, I can report that my energy levels are now very stable, which suggests to me that my glucose levels (whatever they are) are pretty flat.
I do see the appeal to this. It’s convenient to never feel like I have to eat right now. It’s convenient to not feel tired and sleepy after every large meal.
The originator of the two-week test that I’m following, Phil Maffatone, is all about burning fat to power endurance exercise—ultra-marathons and the like.
A body well-adapted to using glycogen for endurance exercise can store maybe 500 grams of glycogen in the muscles and liver combined, providing around 2000 calories. By itself, that’s not even enough to run a marathon, let alone a longer endurance event.
Even a very lean person, on the other hand, probably has at least 10% body fat. That would imply that a 70 kilogram athlete would have around 7 kilos of fat, providing a staggering 63,000 calories. Even allowing for the significant fraction of irreducible fat (cushioning for your eyeballs, etc.) that’s still enough to power literally hundreds of miles of walking or running.
The idea that I’ll be able to do my long runs and very long walks without needing to make special provisions for food is especially appealing.
My glucose levels during the test are in any case only of academic interest. After the test I’ll reintroduce carbs and see how much and what kinds I can eat while preserving the stable energy levels. What I care about is what my glucose levels will be then.
Blood pressure
My blood pressure hasn’t shown much of a trend. So far it’s a little erratic, but has not been down enough to suggest that a different dose of lisinopril is in order. I’ll continue to monitor it.
Allergy symptoms
My allergy symptoms are the thing I’m most interested in improving, and here the results have been at least mildly interesting. I quit taking the Claritin just two days into the test, and then quit taking the Nasacort two days after that. I’m a little sniffly, but I’m not sneezing much, nor am I suffering from the nasal congestion that I needed to take the Nasacort for.
Of course this is not necessarily due to the diet. My allergy symptoms have always been seasonal (even as the “seasons” have grown to cover most of the year); maybe this is just one of the seasons when I’d have been okay anyway. Still, I’d be surprised if that were true. Tree-pollen season has always been a problem for me, and looking out my window, I can see several different kinds of trees with the discreet flowers characteristic of wind-pollination.
Only time will tell, but I’m glad to have at least a few days off the drugs in any case.
I’ll post another update in a week or two, unless the results seem boring.